
-min")
I learned the hard way that pain, and my reaction to it, is one of the useful signals a therapist uses to evaluate the progress of your rehabilitation.
… in the shoulder. What I mean to say is that sometimes physical therapy can be a little painful.
Before I get into too much trouble, let me explain.
My trail back runs through the gym.
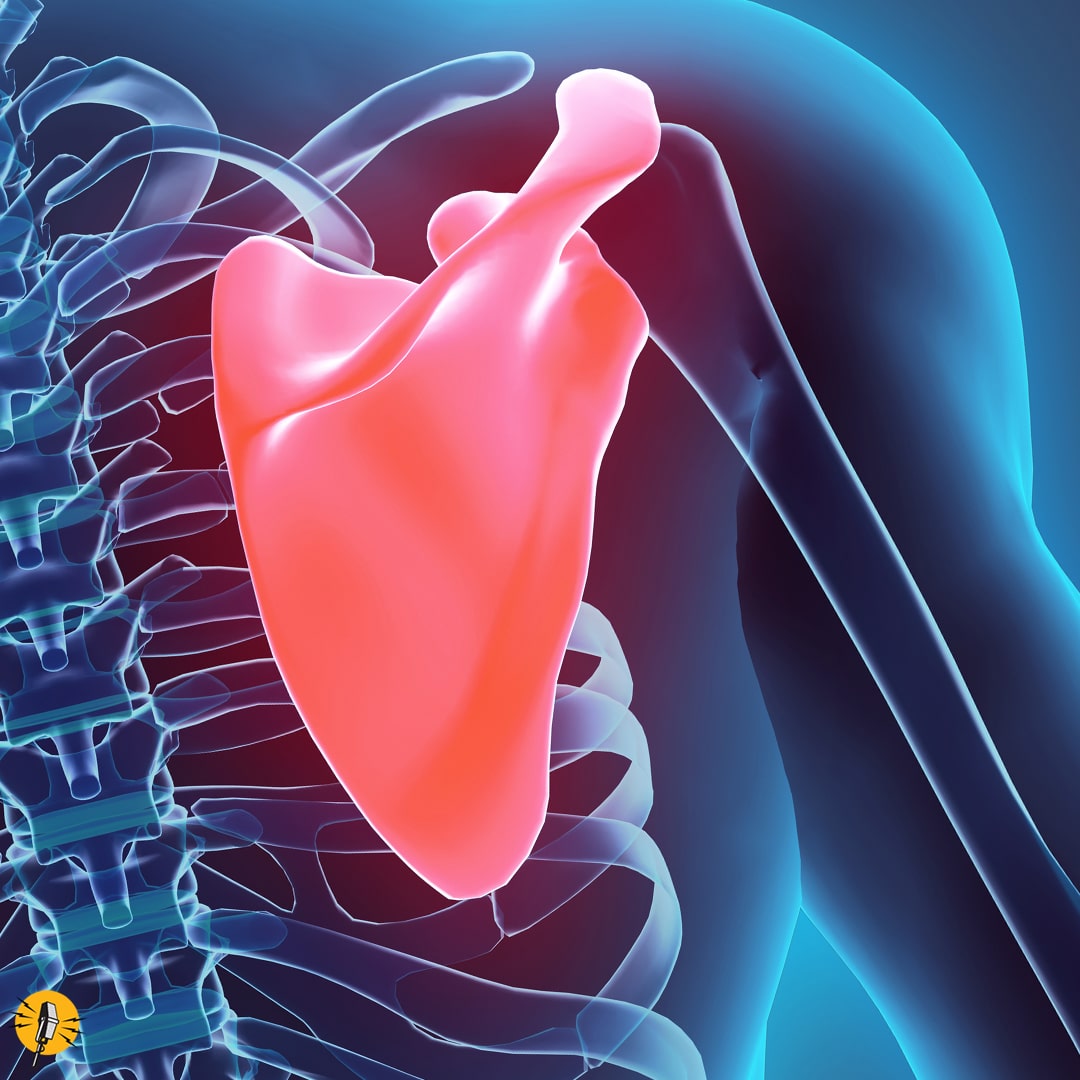
The scapula (also called the “shoulder blade”) is paper-thin and can break. But shattering it is fairly rare.
I knew that at some point, I would have to start exercising my shoulder if I wanted to recover fully. The way it was explained to me, I’d need to give my body time to heal first. Then, I would have to strengthen my shoulder and get as much motion and flexibility back into the joint as possible. Once that was accomplished, my orthopedic surgeon would take a closer look at the remaining damage resulting from my accident.
Getting better can be tough work.
My fall last October shattered my scapula. And even though that paper-thin bone would eventually grow back together, I needed to keep working on the joint to ensure I regained most of my arm’s motion.
Of course, that has meant lots of exercising and stretching. Three days a week, I’m at ORA’s clinic in Northwest Davenport, doing my best to push weight around, stretch elastic bands, bounce balls off walls, and a host of other exercises meant to test, tweak, and build up the muscles in my right shoulder as they attempt to resume the job they were performing before they were so rudely interrupted.
As rehabilitation gyms go, the facilities on Northwest Boulevard seem to be well-supplied and maintained, with a variety of machines and equipment. To the untrained eye, like mine, it looks like your regular hotel gym with just one or two pieces of the same equipment and plenty of television monitors. But on closer inspection, you find every piece of equipment – from brightly-colored stretchy band to steel-grey treadmill – has a specific purpose.
Getting back to life takes perseverance (and a little perspiration).
Therapists use these tools of their trade to help patients regain strength and flexibility. The focus is not on building beach bodies but rather on making it possible for people to move again and get back to the things that matter most in their lives.
Achieving that means you have to rediscover muscles that may have lost their tone while immobilized in a cast or sling. Sometimes it means re-learning basic motions and physical tasks – like putting on a winter jacket – that accommodates your limited mobility or weakened condition.
I often see folks working on re-gaining their balance, teaching their body how to stabilize itself again. It can be hard work and failure is a common occurrence. Most folks might get discouraged and give up, resigning themselves to a “new normal” of limited mobility, pain, and frustration.
But these patients are not doing this alone.
Physical therapists are there by their side, doing what they do best: coaching, collecting, and encouraging.
And in my case, gratefully inflicting a little bit of pain.
Yes, there is such a thing as “good” pain.
Yes, a little bit of pain can be a good thing.
If you think about it, pain serves a purpose. It’s how your body tells your brain that something is wrong and that it needs to find some relief. Pain, and your body‘s reaction to it, are some of the useful signals a therapist uses to evaluate the progress of your rehabilitation.

Kathryn Ellsworth, ORA Physical Therapy
When I asked my therapist, ORA Orthopedics’ PT, Kathryn Ellsworth, about my pain signals, and how she used them in my therapy, she explained it this way:
“I monitor both non-verbal and verbal reports of pain and adjust my therapy accordingly. I know that what we do is going to produce some discomfort because we’re trying to address the damage to the joint and surrounding soft tissue. But I’m careful because causing too much pain can be counter-productive and could be hard to relieve.”
So … it could be worse. I guess I should stop complaining about being so sore all the time.
“Some people confuse the two. There is actually a big difference between soreness resulting from muscle fatigue after a rehab session and pain caused by some kind of trauma a person has suffered – like falling ten feet onto a cement stone.”
Okay, I kind of deserved that.
My therapist can read me like a book … and it’s probably Dr. Seuss.
So, apparently, my reactions to the aches and pains I suffer through during my therapy (usually consisting of grimaces and bad Dad-jokes) are just part of what Kathryn takes into consideration as she’s guiding my recovery. She observes how these verbal and nonverbal cues compare to what she’s feeling inside my shoulder as she works it through a series of motions.
As the shoulder begins to resist the pressure to move, Kathryn looks to see if I’m expressing some level of pain. And I usually am. An eye roll might mean one thing. A wince or a muffled scream might mean something else.
Actually, I rarely scream during physical therapy because 6:15 am is far too early in the morning for that kind of behavior – and I’ve only had one cup of coffee, so I’m only half awake.
In reality, the pain isn’t usually too severe. Kathryn will push or pull on my arm and my shoulder will sometimes tweak or twinge. It can be a sudden snapping sensation, like someone shooting my shoulder with a rubber band. If not that, I’ll experience a dull, throbbing sensation – like when my arm feels it isn’t fully back in the shoulder socket – which it isn’t.
Kathryn compares her knowledge of physiology with my description of how things feel and creates a new data point to track my recovery.
My trail back will be a long one. And I knew that at times it would be painful as well. But it’s good to know all the pain serves a purpose.
The trail doesn’t end in pain … at least it doesn’t have to.
It’s also good to know that there are ways to deal with the pain that goes beyond taking a dose of “Vitamin I“ (that’s how ORA PA, John Tyron, referred to ibuprofen during my last visit).
But that’s a story for another day. I hope you’ll stay with me on this trail as we go down it together.

A dream job … or just a job of dreams?
You need to know one of the true “wizards” of Disney’s Imagineering department. He’s made a real-life lightsaber and now he’s creating the technology that could put a Holodeck experience in every home. Find out more …

So long Leap Day, see you in 4 years (or so) …
Oh sure, it seems obvious. Every four years, we’ll just add an extra day to the calendar. Unless the year ends in a 00, then … well … read this post and you’ll know all you really need to know about “Leap Days.”

Gone but not forgotten – favorite automotive trends from the past
America (and much of the world) has had a century-long love affair with automobiles – of all shapes and sizes. But just like that person you dated back in high school, a second look few decades after the fact may result in a raised eyebrow or two.

Leaping back into the DAILY SPAM … and much more.
It’s well preserved in its own juices and fresh out of the can. The DAILY SPAM is back.

Celebrating the best underwater photography of the year
The online gallery showcasing the best entries of the 2024 Underwater Photographer of the Year competition is absolutely stunning. I’ve posted a few samples and a link to the online exhibit.

Nothing to watch on HULU? Not exactly …
Overwhelmed with options when it comes to finding a new series to stream or a movie to watch? If you’ve got a subscription to HULU, I might have a few suggestions …

How Godzilla found his voice
There’s something delightfully nostalgic about the unforgettably corny schreech of a roar coming from the original King of the Monsters (Godzilla) in the original 1954 production. Here’s the story behind the sound …

Additions for your “ttrbyd” list
What’s this? Just another one of those lists of things to do, read, watch, experience before you leave this mortal coil? Maybe, but it’s worth the read.

A little walk can take us miles
How many steps do you take in a day? Believe it or not, there are physiological, mental, and emotional benefits to literally “taking a hike” whether your wife asks you to or not.

Apple’s big bet on the MLS
How does Apple view its 10-year, $2B+ deal between Apple TV+ and Major League Soccer? It’s a way to reinvent sports for a streaming environment and get in on the ground floor of what could be the freshest source of “reality television” on the planet.

Animal stories … and much more.
Whether it’s a rampaging bear, a happy dog, or the return of the woolly rhino … it’s all good in today’s DAILY SPAM.

Still turning heads at 50 … happy birthday to THE EXORCIST.
Everything from celebrating fifty years of head-spinning thrills to the health benefits of ice cream. It’s all part of today’s nutritious meal of email delights.

Have you had your SPAM today?
Introducing a new column … Daily Spam is what I serve up after digging through the hundreds of emails I get every day … just so you don’t have to. I’ll provide links to interesting articles, videos, podcasts and more with no offers for winning lotto numbers, inheritances from African princes, or the latest NFTs. It’s free content worth every penny. Guaranteed.

You’ll never guess where I found the biggest obstacle to my recovery journey …
It turns out that the mind-body connection works both ways. Sometimes the biggest barrier keeping you from your success is located between your ears – which is why its important to understand how physical trauma can bring on depression and how your mental health affects your recovery.

The patient can go on vacation, but the therapy can’t.
Even when you intentionally “get away from it all” you don’t get away from it ALL. Blogger Mike Bawden explains how to manage travel, touring foreign countries, chasing grandchildren, and rehabbing an injured shoulder simultaneously.